

Tag: givewell
-
Casting a Wider Net for Cost-Effective Programs
GiveWell tends to be known for its work in areas like malaria prevention, water treatment, and nutrition. But as our research team has grown, so has our ability to search for cost-effective programs across a much wider range of issues. Serious health problems, such as lack of medical oxygen and stockouts of essential medicines at…
-

June 2026 updates
Every month we send an email newsletter to our supporters sharing recent updates from our work. We publish selected portions of the newsletter on our blog to make this news more accessible to people who visit our website. For key updates from the latest installment, please see below! If you’d like to receive the complete…
-
Looking Back to Give Better: A Webinar Recap
GiveWell’s latest webinar took a close look at a critical step in our research process: how we’re working to evaluate past grants to understand what happened, why, and how we can use what we learn to improve our grantmaking over time. Our research spans the full lifecycle of grants. Before we approve funding for a…
-
Expanding Our Search for Cost-Effective Ways to Reduce Poverty
In September 2025, we created a livelihoods research subteam to specifically focus on programs that increase the economic well-being of people in extreme poverty. While we have evaluated and funded livelihoods programs throughout GiveWell’s history, we now have a dedicated program officer overseeing this portfolio, which has allowed us to build on and deepen that…
-
Growing GiveWell’s Largest Research Area: Malaria
Despite significant progress fighting malaria over the past few decades, the disease still kills around 600,000 people annually. Malaria is a leading cause of death globally, especially for young children in Africa, who make up around 70% of all malaria deaths worldwide.1See the WHO fact sheet on malaria, which states “Globally in 2024, there were…
-
Building our Safe Water Grantmaking: Apply to the DIV Fund’s RFP
GiveWell has granted $5 million to the DIV Fund to identify and support promising water quality and access innovations. Our grant aims to build a pipeline of high-potential, cost-effective opportunities that GiveWell could consider for future funding. If you’re working on piloting or testing an early-stage water intervention, or know someone who is, please apply…
-
May 2026 Updates
Every month we send an email newsletter to our supporters sharing recent updates from our work. We publish selected portions of the newsletter on our blog to make this news more accessible to people who visit our website. For key updates from the latest installment, please see below! If you’d like to receive the complete…
-
How We’re Searching for the Best Ways to Help in 2026
This year, our research team is focused on two primary goals. The first is to rapidly scale our capabilities so we’re able to move much more donor funding to highly cost-effective programs in the near future. The second is to grant at least $500 million to the best opportunities we can find this year to…
-
Podcast Episode 29: Behind the Analysis — Assessing Past Malaria Nets Grants
GiveWell’s research doesn’t end once we’ve made a grant. We evaluate a subset of completed grants, comparing what we thought would happen to what actually took place, then try to use what we learn to improve our future funding decisions. Over the past year, we’ve formalized and expanded this work, publishing comprehensive “lookbacks” for select…
-
GiveWell Opens RFI for Malaria Pilots and Research
GiveWell is launching a new request for information (RFI) to expand and strengthen our malaria grantmaking in Africa and help our donors make a greater impact. Expressions of interest can be submitted through one of two tracks, the first for malaria chemoprevention and vector control pilot programs and the second for research and evaluation. Submissions…
-

April 2026 Update
Every month we send an email newsletter to our supporters sharing recent updates from our work. We publish selected portions of the newsletter on our blog to make this news more accessible to people who visit our website. For key updates from the latest installment, please see below! If you’d like to receive the complete…
-
Podcast Episode 28: Evaluating and Funding a New Kind of Grant (Clubfoot Treatment)
Clubfoot, a congenital condition where children are born with one or both feet twisted inward, affects roughly one in 800 newborns globally. Most of those cases are in low- and middle-income countries, where only about 20% of children with clubfoot receive treatment. While most donations to GiveWell are directed to programs that reduce child mortality,…
-
Podcast Episode 27: Scrutinizing One of Our Longest-Funded Programs
Vitamin A supplementation is one of the programs GiveWell has supported the longest, and we’re currently funding it in many African countries. The program has an unusually strong evidence base for reducing child mortality, with multiple randomized controlled trials. Yet, as is the case for most global health programs, the evidence for vitamin A supplementation…
-
March 2026 Updates
Every month we send an email newsletter to our supporters sharing recent updates from our work. We publish selected portions of the newsletter on our blog to make this news more accessible to people who visit our website. For key updates from the latest installment, please see below! If you’d like to receive the complete…
-
Podcast Episode 26: Investing in Information for Greater Future Impact
GiveWell’s primary focus has always been researching, identifying, and directing donations to programs we believe will do the most good. When GiveWell first started, we approached this by looking for organizations that were already delivering highly cost-effective, evidence-backed programs and directing funding to those programs. Over time, we were able to focus further upstream by…
-
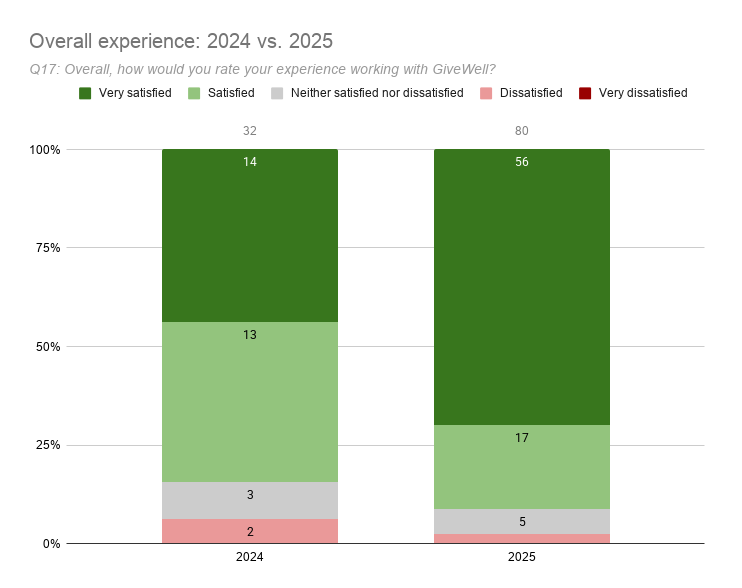
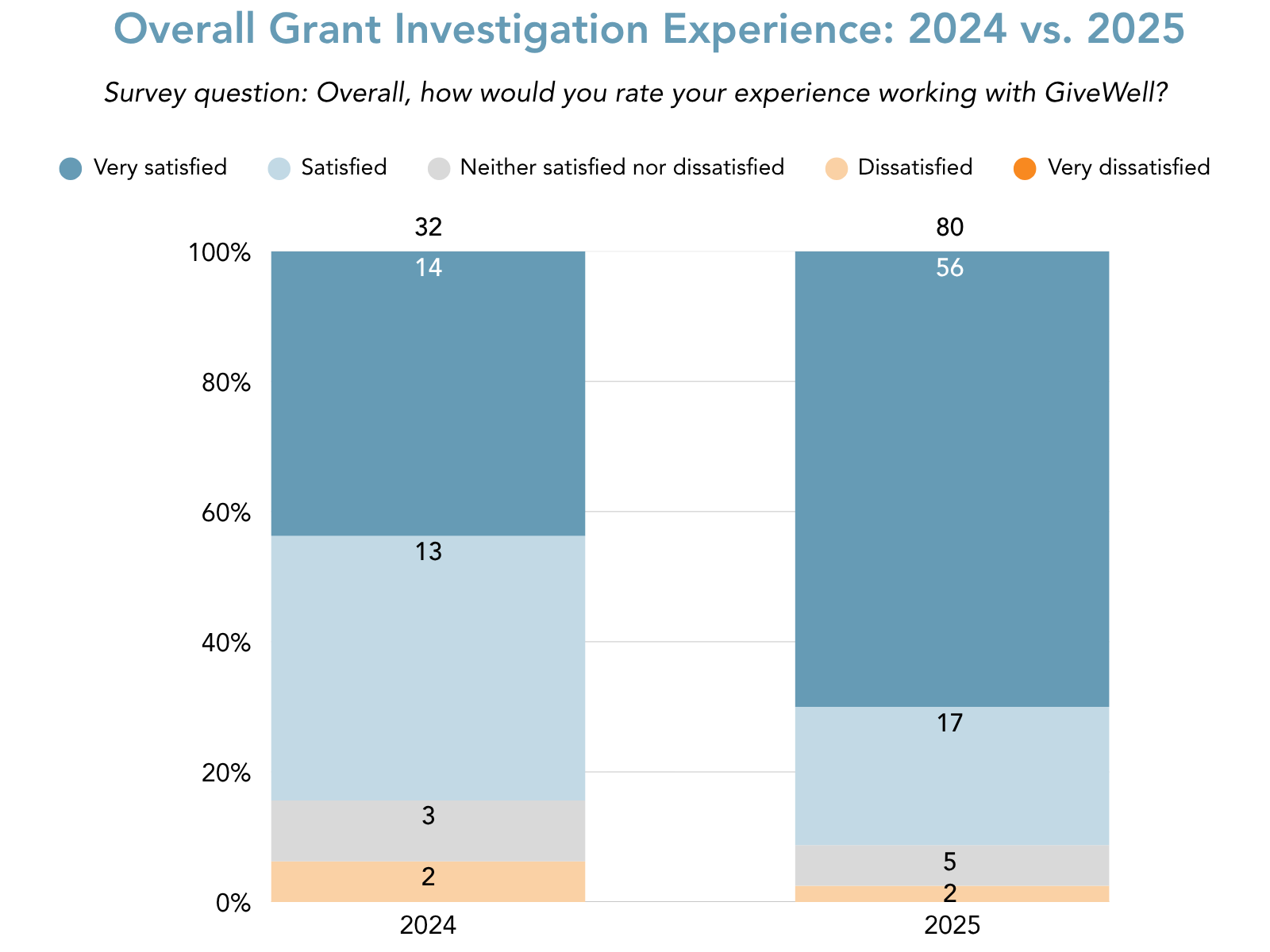
GiveWell’s 2025 Grant Investigation Survey Results
Over the past several years, GiveWell has been focused on growing, deepening, and improving our research team’s work in line with our core values of truth-seeking and transparency. As part of that effort, we’ve invited anonymous assessment of our grantmaking process in order to learn and improve. In July 2024, we sent out our first…
-

Podcast Episode 25: Following the Data on Dispensers for Safe Water
GiveWell aims to find and fund programs that will do the most good per dollar. To do this, we carefully evaluate potential grants before making them—assessing academic evidence, building cost-effectiveness models, and talking to people in the sector who know the program well. But our work doesn’t stop there. When a program we’ve supported nears…
-
February 2026 Updates
Every month we send an email newsletter to our supporters sharing recent updates from our work. We publish selected portions of the newsletter on our blog to make this news more accessible to people who visit our website. For key updates from the latest installment, please see below! If you’d like to receive the complete…
-
GiveWell Launches RFIs for Targeted Vaccination Outreach in Three Countries and Anemia Control Programs in Africa
GiveWell is launching two new requests for information (RFI) to expand GiveWell’s funding for vaccination outreach and anemia control programs. We’re excited to replicate the success of last year’s water chlorination RFI and explore how to reach even more people in low- and middle-income countries with programs to save and improve lives. The first RFI…
-
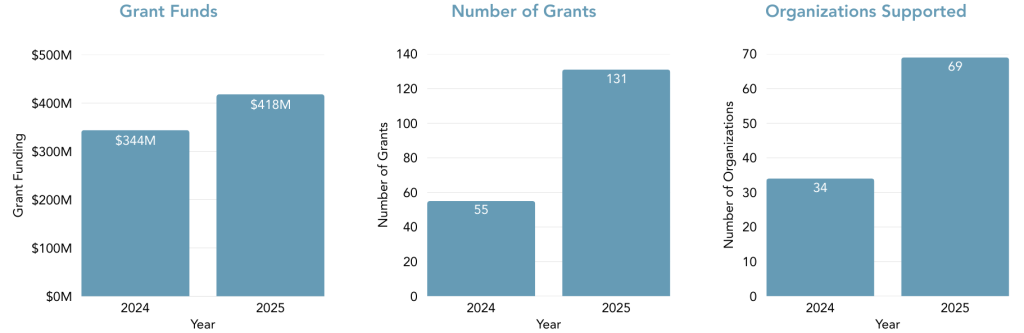
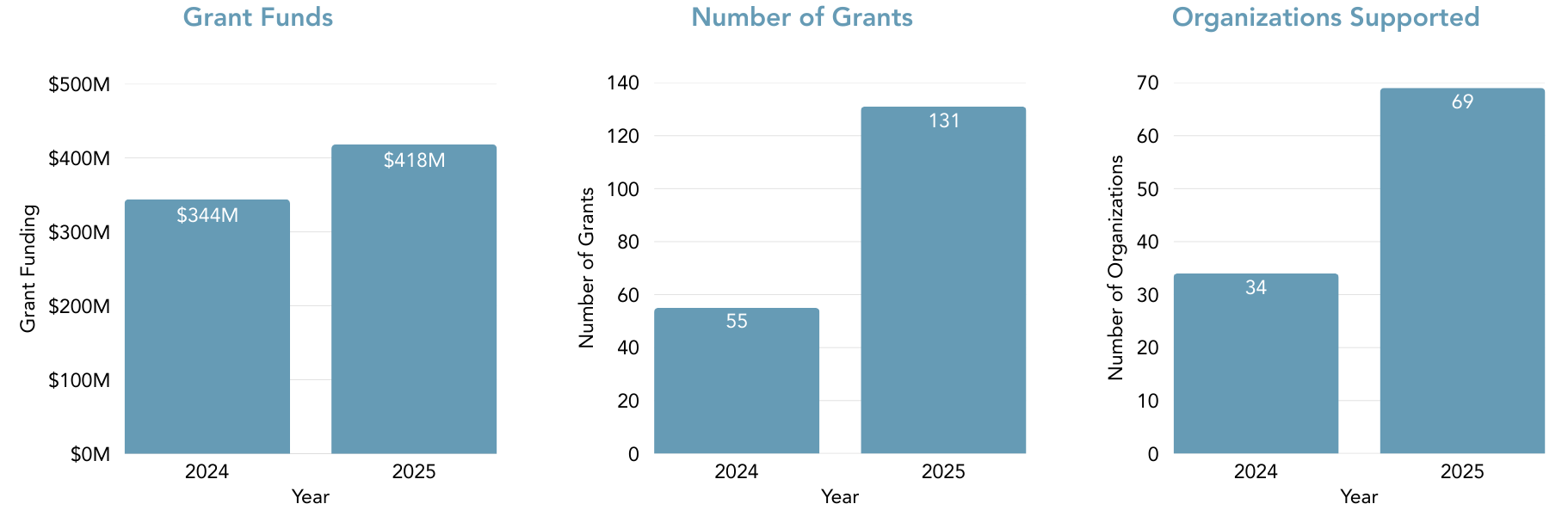
GiveWell’s 2025 Grantmaking: Record Grants, Expanded Reach, Crisis Response
In our 2025 grantmaking year, GiveWell approved $418 million in grants to highly cost-effective programs in order to save and improve lives as much as we can. Through years of deliberate groundwork, we’ve been growing our research capacity and scope in order to direct substantially more funding to the most impactful opportunities we can find.…